
Vial Coring, Ampoule Shards, Reusing Needles - What's the Deal?
The reddit wiki also has comprehensive articles on the topic
https://old.reddit.com/r/TransWiki/wiki/hrt/injections#wiki_coring
https://old.reddit.com/r/TransWiki/wiki/hrt/injections#wiki_filter_needles
Vial coring
Injectable medications are often supplied in the form of vials. Vials have a rubber top crimped on with a metallic cap. A needle can “core” the vial by cutting out a piece of the rubber during insertion. This is an issue because (1) it may result in the accidental injection of the rubber piece and (2) it may allow bacteria or pyrogens to enter the vial.

18G needles are often used as “drawing needles” for the medication (the needle subsequently being replaced by a higher gauge one prior to injection). One study1 investigated the rate of coring in propofol vials using different gauge needles and concluded that “Large-bore needle was the factor that impacted rubber coring after puncturing through the rubber stopper of the multi-dose vial, regardless of the angle of puncture.”
Blunt needles are sometimes recommended for injection also. To quote a forum user2:
I believe you are suppose to use a blunt fill needle to draw up, it’s less likely to cut the rubber. It’s just hard to pull up a large amount quickly through it
Another study3 investigated the incidence of coring with blunt versus sharp needles.
Rubber caps were then pierced with either an 18-gauge sharp hypodermic needle or a blunt plastic (safety) needle. Coring occurred in 102 of 250 (40.8%) vials when a blunt needle was used versus 9 of 215 (4.2%) vials with a sharp needle (P < 0.0001).

Welp, evidently the forum user was wrong. I don’t have a medical background but in my time researching medical topics I’ve noticed on multiple occasions “standard practice” contradicting technique efficacy studies, this being a good example. I wonder if this is due to aspects of medical practice that haven’t been taken into account in the studies, but I suspect it is simply a result of historical convention and maintaining the status quo at medical schools (someone with actual medical experience might have better insight here).

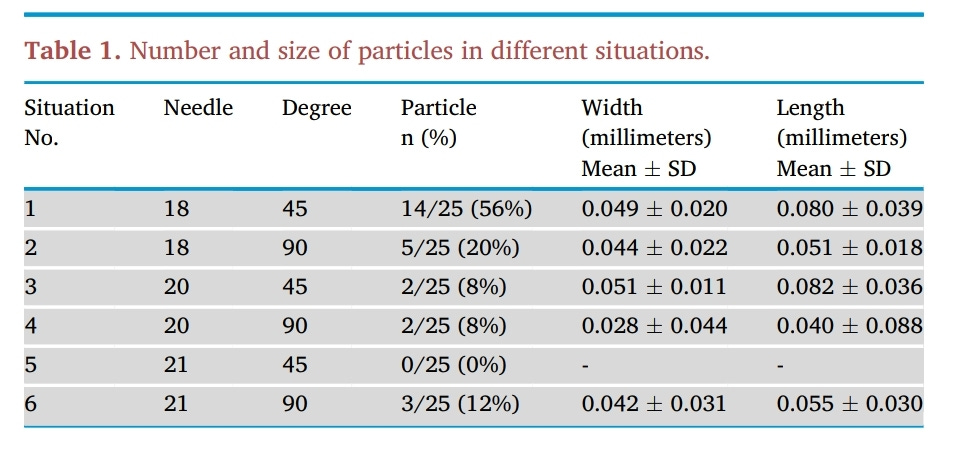
The rate at which cored vial particles were subsequently ejected from the needle has also been investigated4.
Prednisolone acetate (Hydrocortancyl, 125 mg; Sanofi-Aventis, France) was drawn up through the rubber bung of the vials with an 18-gauge cutting bevelled needle. Medication was drawn up using the recommended technique of needle insertion into a medication vial that reduces the risk of coring. The needle was inserted at a 45–60° angle, with the opening of the needle tip facing upwards.
Coring occurred in 21 of the 200 samples (10.5 %).
After injecting 3 ml of the medication containing a core through a 20-gauge spine needle, we detected that in 1 of the 21 cases (4.7 %) the core was ejected through the needle.
We therefore speculate that coring may often go undetected and thus represents an under-reported problem that healthcare providers need to be aware of.
Incidence is small but not negligible! Definitely something to be avoided.
Ampoule shards
In the case of ampoules, glass shards are also an issue5.
The results of our study showed that, out of 510 glass ampoules, a total of 113 glass particles were found, giving an average of 0.22 particle per ampoule. When sampled ampoules with matching wall thickness (0.70–0.80 mm) and type (metal-etched) were compared, we found that those with a larger size (larger than 2 ml capacity, n=13) have a greater averaged number of glass particles per ampoule (0.46), compared to that of smaller ampoules (0.14), where n=162. For sampled ampoules with matching wall thickness (0.80–0.90 mm) and size (larger than 2 ml capacity), we found that metal-etched ampoules (n=55) have a greater averaged number of glass particles per ampoule (0.47), compared to that of colour-break ampoules (0.24), where n = 93. These results are in concordance with other studies [2,3].
To minimise administering glass particles to patients, we recommend either the use of in-line filter, or aspiration through a fine-bore needle as well as avoiding aspiration from the most dependent area of the glass ampoule.
One study6 investigated effect of ampoule opening technique on quantity of glass particles and concluded that “breaking an ampoule with a cotton ball from an outward direction resulted in the fewest glass particles.” Nonetheless the variation in quantity of particulates was not that large.
I found another good article7 on the topic that concludes essentially the same thing as most other sources - realistically speaking the risk is just very low.
Reusing needles
There is an image that gets passed around the interwebs and textbooks a lot:

The image is cute but misleading. If we rescale the last image to be the same magnification as the first and overlay them we get:
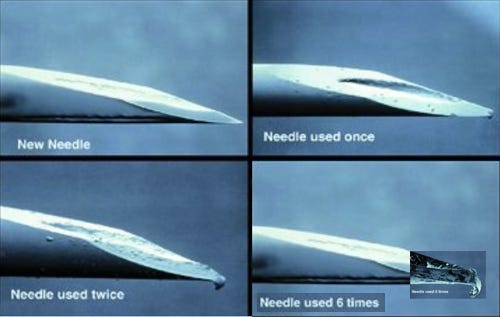
I tried to look for the original source of these images, alas without success. Anyways, reusing needles isn’t actually that bad in terms of needle degradation8, its bad because of contamination risk etc. etc.
Unused needles could be differentiated visually from used needles. However, there was no correlation between the actual and guessed number of times a needle was used (r = 0.07, P = 0.2). Evaluating all 270 injections, neither pain intensity nor unpleasantness increased with repeated injections of the same needles in people with diabetes (P = 0.1 and 0.96) and in the volunteers (P = 0.63 and 0.92).
Using pen needles four to five times does not lead to progressive needle tip deformity and does not increase pain intensity or unpleasantness, but could increase convenience and lead to substantial financial savings in Europe of around EUR 100 million/year.
Thus there should be no any issues with using the same needle for drawing from a vial and performing the injection, as long as no coring occurs (assuming also that you sterilise things properly - wipe down your hands and the vial with alcohol, use a sterile needle straight from the package etc).


Conclusion / TL;DR
If you want to be careful, probably use a filter drawing needle and a separate needle for injection, both for ampoules and vials.
Do not use an 18G drawing needle, especially not a blunt one. In my experience, reusable vials are more convenient than glass ampoules, and probably marginally safer, but ultimately its personal preference.
The risk of glass shards from ampoules or rubber particles from cored stoppers is small, especially when using a needle smaller than 20 gauge. Use the injection needle (>25G) for drawing and you will be fine!
Don’t just trust what I say, read the research yourself and make your own conclusions :)
Chotikawanich T, Kammee T, Khantee S. The impact of needle size and angle on rubber coring after multiple puncturing of multi-dose propofol vial rubber stoppers. Heliyon. 2022;8(5):e09389. doi:10.1016/j.heliyon.2022.e09389
https://forums.studentdoctor.net/threads/little-bits-of-the-propofol-stopper.1412999/
The incidence of coring with blunt versus sharp needles. J Clin Anesth. 2014;26(2):152-154. doi:10.1016/j.jclinane.2013.10.007
Campagna R, Pessis E, Guerini H, Feydy A, Drapé JL. Occurrence of coring after needle insertion through a rubber stopper: study with prednisolone acetate. Eur Radiol. 2013;23(2):424-427. doi:10.1007/s00330-012-2602-3
Lye ST, Hwang NC. Glass particle contamination: is it here to stay? Anaesthesia. 2003;58(1):93-94. doi:10.1046/j.1365-2044.2003.296812.x
Chiannilkulchai N, Kejkornkaew S. Safety concerns with glass particle contamination: improving the standard guidelines for preparing medication injections. Int J Qual Health Care. 2021;33(2):mzab091. doi:10.1093/intqhc/mzab091
https://trthub.com/broken-glass-in-ampoules-the-risks-and-how-to-avoid-harm/
Puder JJ, Atar M, Muller B, Pavan M, Keller U. Using insulin pen needles up to five times does not affect needle tip shape nor increase pain intensity. Diabetes Res Clin Pract. 2005;67(2):119-123. doi:10.1016/j.diabres.2004.06.001
i still send this article to friends when discussing DIY, so i wanted to come here and thank you for your hard work writing it :) much appreciated